| Want to send this page or a link to a friend? Click on mail at the top of this window. |
| More Books and Arts |
| Posted November 25, 2007 |
|
||
 |
||
PETER VAN AGTMAEL/POLARIS |
||
| IN THE STORM An H.I.V. support group walks past and AIDS ribbon in Lesotho, Africa, in 2005. |
By DONALD G. McNEIL Jr. |
IGNORE the fuss over the news last week — the United Nations’ AIDS-fighting agency admits to overestimating the global epidemic by six million people. That was a sampling error, an epidemiologist’s Dewey Defeats Truman.
Look instead at the fact that glares out from the Orwellian but necessary revision of the figures for earlier years. There it is, starkly: AIDS has peaked. New infections reached a high point in the late 1990’s — by the best estimate, in 1998.
There must have been such moments in the past — perhaps A.D. 543, when Constantinople realized it would survive the Plague of Justinian, or 1351 in medieval Europe, when hope dawned that the Black Death would not claw down everyone.
Eleven years ago, there was a milestone moment in AIDS history when Andrew Sullivan wrote an article in The New York Times Magazine titled “When Plagues End.” It argued that a new treatment, the triple therapy cocktail, meant it was finally possible to envision AIDS as a chronic illness, not an inevitable death sentence.
 |
EVELYN HOCKSTEIN/POLARIS |
| SOLACE Anthony Okello, a traditional healer who studied under a wandering witch doctor, tends to an AIDS patient in Apac, Unganda in 2006 |
Naturally, he was, in his words, “flayed alive” by the AIDS establishment. An end in sight implied that vigilance could relax — although he hadn’t actually argued that.
Mr. Sullivan’s view was solipsistic. It celebrated hope for gay American men still reveling in their sexual freedom and barely mentioned the wider reality of newborn babies and faithful wives in Africa who were never to enjoy any freedoms and still were doomed to die miserably in numbers that would blast the exit doors off every gay bar in North America.
Now, out of the mists of the old data, another such moment has emerged, one for the worldwide stage.
The first thing experts are again quick to say is that it doesn’t mean anyone can relax.
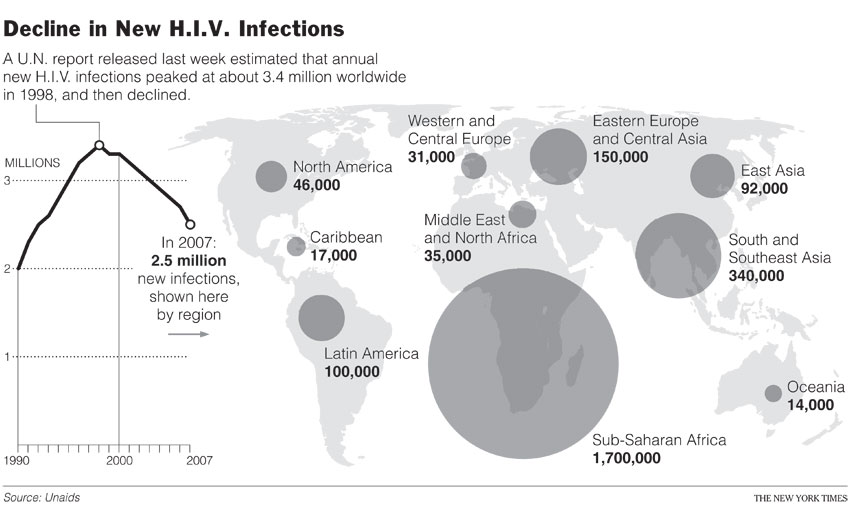 |
More than three million annual new infections in 1998, or an estimated 2.5 million for 2007, “is not a particularly happy plateau,” said Dr. Robert Gallo, a discoverer of the AIDS virus.
Dr. Mark R. Dybul, the Bush administration’s global AIDS coordinator, added: “I don’t think it radically shifts our thinking, at least not for 5 to 10 years. We still need to prevent 2.5 million infections, we still need to prevent 2.1 million a year from dying.”
Nonetheless, the disease is at last giving notice that it will behave like other pestilences.
AIDS has always been maddening. It moves more slowly than anything that rides sneezes or coughs or rats or mosquitoes. It permits years of symptom-free infectivity and kills, like a torturer, at its leisure.
Classically, all epidemics first strike down those in the vanguard: the Genoese merchants who fled the siege of Caffa in 1347, bringing plague to Europe; the conquistadors who “discovered” syphilis in the New World. If an avian flu pandemic emerges, it will be among poultry farmers and kindergarten teachers, who both herd flocks of little vectors. In gay America, it was flight attendants and rent boys.
Then epidemics typically surge into pockets where conditions are perfect: ports teeming with rats; populations weakened by famine; flooded Bengali streets; Thai brothels.
Finally, inevitably, they begin to burn out. Hosts die faster than new hosts can be found. And, crucially, the hosts get smarter. They flee cities, drain swamps, invent vaccines or accept self-restraint and condoms.
Until now, AIDS had defied that paradigm. Its dark spiral seemed to just keep widening — central Africa was worse than America, southern Africa was worse than that, India would be worse, China was next
But it now appears that the burnout has been underway for years.
In the year 2000, I wrote an article for this section trying to calculate how much it would cost to contain global AIDS, which was said to infect 30 million people in poor countries. (Last week’s revision drops that closer to 23 million.)
Officials of Unaids, the United Nations’ agency, declined to be quoted saying so at the time, but in their policy decisions, they had written off all who were already infected.
The agency was seeking $2 billion a year for Africa — simply for prevention. Triple therapy cost $12,000 a year per patient. Cipla Ltd., the Indian generic-drug maker, had not yet offered to supply the drugs for $350, which set prices tumbling; they are now $150. The Global Fund to Fight AIDS, Tuberculosis and Malaria did not exist.
Undoubtedly, virtually all of those 23 million are now dead. Even now, most could not be saved — antiretroviral drugs reach only about one-tenth of those who need them.
But now we know that those falling legions were right at the cusp of the epidemic. Albeit imperceptibly at the time, things were improving. The sight of so many skeletons had scared a lot of Africans into changing their habits.
It’s still not clear why southern Africa was hit the hardest. There are theories — migratory mine labor, less circumcision, perhaps a still-undiscovered genetic susceptibility.
But the southern Africa explosion has not repeated itself as the virus moved on into Asia’s much greater populations. It has hit very susceptible pockets, like the red light district of Calcutta, but seems to have stalled in them.
“In the 90’s,” said Dr. Paul De Lay, director of monitoring and policy for Unaids, “we thought that if you had the crude signs that risky sex was going on, like brothels or refusal of condoms, then any country could erupt into a generalized epidemic. That’s not true any more. Now we’d never say China is likely to have an African-style epidemic.”
This does not mean that shrinking numbers are inevitable.
The disease is still rooting out new pockets; infections are rising in Vietnam, Uzbekistan and even Indonesia, the world’s fourth-most-populous country.
It can also lull its hosts into acting foolishly again; that has happened in San Francisco and Germany, Dr. De Lay noted, where new infections are ticking up again as young gay men revive the bar scene of the 1980’s.
And, Dr. Gallo warned, a mutation — a virus more easily transmitted or more drug resistant — could emerge. Epidemics traditionally move in waves; that could trigger a second.
Nonetheless, the new estimates mean the vision Mr. Sullivan had of the American epidemic is now possible for the global one: a day when AIDS is viewed as a chronic problem, another viral predator taking down the careless or weak members of the herd, as pneumonia takes down the old ones.
Also possible in the future — the very distant future, Dr. Dybul warned — is a day when the calculation I tried to do will have an answer that is actually affordable.
After all, even the Black Death is not dead. But it is cornered, and very cheaply. Its cause, Yersinia pestis, lives on in fleas and rodents, and there are about 2,000 cases each year, a handful of them in the American Southwest. But penicillin kills it.
Nothing yet kills AIDS. When that day comes, another rewrite of the epidemic’s history will begin.
Copyright 2007 The New York Times Company. Reprinted from The New York Times, Week in Review, of Sunday, November 25, 2007.
| Wehaitians.com, the scholarly journal of democracy and human rights |
| More from wehaitians.com |